Custom Intramedullary Femoral Arthroplasty with Hyperextension Knee Joint
Case Report: directLINK 1/2024
A 42-year-old female patient presented with a complex medical history including primary biliary cirrhosis and multiple epiphyseal dysplasia. Her previous surgical procedures included a primary right total knee arthroplasty (TKA) followed by a revision TKA with the LINK Endo-Model XS implant system. She also underwent a patellectomy due to skin problems in the anterior knee. Additional complications included a periprosthetic femoral fracture and subsequent periprosthetic joint infection. This case report discusses the challenges and the multidisciplinary approach required for successful treatment.

The post-operative X-ray shows the correct fit of the intramedullary femoral total knee arthroplasty with hyperextension knee joint, developed by customLINK.
The first stage of the surgical procedure consisted of two major steps: removal of the distal femur, a tibial tuberosity advancement osteotomy (TTA), and an additional osteotomy in the tibial half in preparation for implantation of the intramedullary femoral and tibial components.
Various surgical challenges
Because the patient had multiple orthopedic complications, surgical intervention with custom implants was required. The goal was to optimize functional outcomes while addressing the patient’s unique physical and clinical limitations.
Multiple requirements for the customLINK manufactured implant
customLINK was asked to develop an implant that would address the fact that limited range of motion made arthrodesis inappropriate (reliant on wheelchair), while the lack of a functional extension mechanism precluded conventional joint replacement. Anatomical limitations such as a small tibial metaphysis and narrow femoral canal made implant fixation difficult. Additional factors such as increased risk of infection, nickel allergy, and dermatologic limitations (no skin grafting possible) further limited surgical options. Overall, the case required careful planning and specialized approaches to overcome the numerous obstacles to standard treatment.
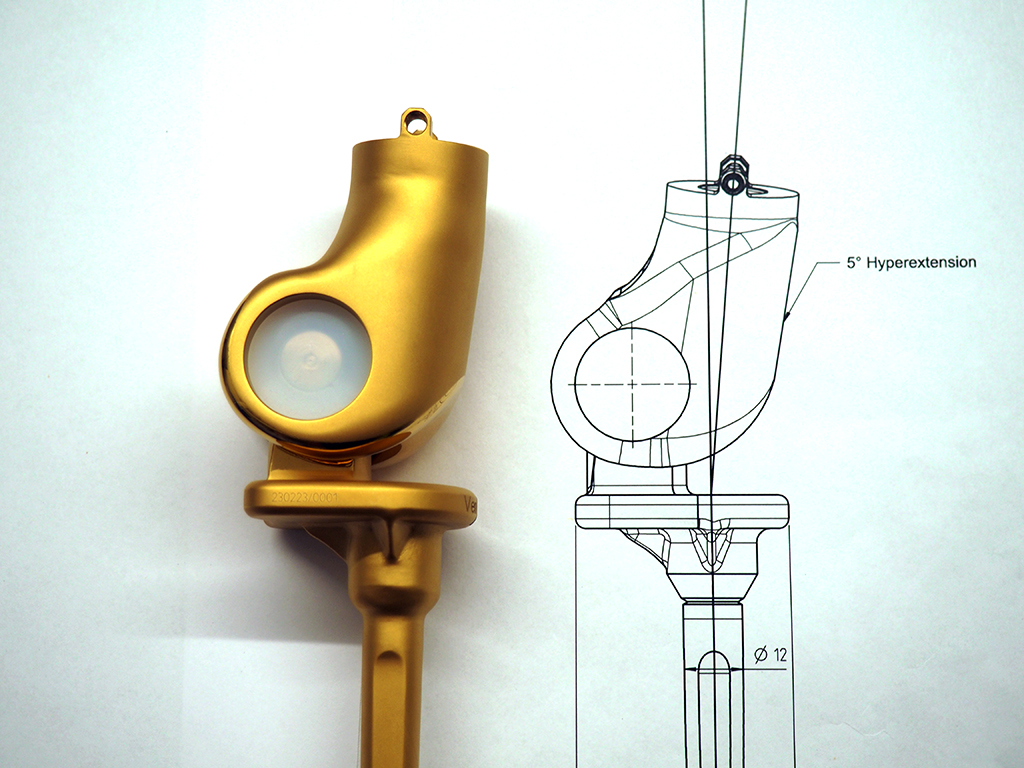
customLINK’s development of a 5° hyperextension hinged knee with intra-medullary femoral nail in the knee joint solved the challenges of the narrow femoral canal and fixation issues. The choice of an extra narrow hinge design was intended to accommodate the anatomical constraints, and the hyperextension joint design allowed for some recovery under load.
The monobloc tibial component with a long tibial stem was designed to accommodate the small tibial metaphysis and provide more secure fixation. On the femoral side a modular anatomical push-through stem connects proximally a short MP neck segment and distally a support ring, stem segments and the total knee joint replacement.
Coating options for biocompatibil-ity and infection control
Coating options such as LINK PorEx and LINK PorAg offer advantages in terms of biocompatibility and infection control.
In summary, the specialized surgical components, including the total intramedullary femur, the extra narrow hinge design, the push-through stem option and the monobloc long stem tibia, have been designed to meet the complex anatomical and functional requirements of the patient. LINK PorEx and LINK PorAg coating are applied to address the specific challenges of infection risk and biocompatibility of the material.
The intramedullary femoral arthroplasty with hyperextension knee joint was successfully implanted.

LINK Endo-Model XS implant system in situ.

The situation reflects a massive skin lesion due to periprosthetic joint infection.

The radiographs show the situation after distal femur removal, TTA osteotomy and re-osteotomy in the tibial half to align it for the second phase.

The radiographs show the situation after distal femur removal, TTA osteotomy and re-osteotomy in the tibial half to align it for the second phase.

Individual implant components with coating.

Design rationale for customLINK manufactured implant components.