»I immediately had excellent confidence with the LinkSymphoKnee system and the instruments, which led to great postoperative satisfaction« (Dr. Giuseppe Calafiore)
directLINK 2/2023

Members of the development group for the new LinkSymphoKnee include German surgeons Prof. Georg Matziolis and Dr. Alois Franz and Dr. Giuseppe Calafiore from Italy. In this interview they discuss instrumentation, workflow and early clinical results.
Prof. Matziolis, Dr. Franz, Dr. Calafiore:
How does the LinkSymphoKnee stand out from other implant systems?
Prof. Matziolis:
The LinkSymphoKnee exceeds my expectations and impresses me. It works flawlessly right out of the box with no major problems. It is a pleasure to implant the LSK and I have noticed that my colleagues in the clinic also prefer it to other implant systems. I am more than satisfied with the LinkSymphoKnee, I am thrilled.
Dr. Franz:
The LSK system does indeed have many advanced design features that overcome the disadvantages of older systems. The features include the very thin anterior femoral shield, the 4.5 degree anterior cut, and the standard narrow implant. These improvements simplify the surgical process and reduce operating time. The LSK system also features an innovative design that improves patellofemoral joint motion, enhances intrinsic stability during surgery with the PS-Plus system, and covers a complete product range up to the CCK system with cementless or cemented stems, wedges and cones. These versatile options provide real benefits for surgeons and patients.
Dr. Calafiore:
Overall, the outstanding feature of this prosthesis is the technology with which it has been designed and constructed. In its entirety, this technological configuration offers a system for preserving the posterior cruciate ligament, to a configuration with the possibility of increasing levels of constraint in the case of ligament insufficiency, to a fully constrained implant, with a simple and versatile procedure. The wide range of femoral and tibial sizes guarantees a restoration according to the knee anatomy, selecting the most appropriate AP and ML sizes.
What is the impact of the instrumentation?
Dr. Calafiore:
The LSK system’s key strength compared to competitors in the market is certainly the instrumentation. This instrumentation allows not only different implant configurations with fewer surgical trays, but also the possibility of having both a standard and a hypoallergenic version, from the initial implant to the revision. The instrumentation guarantees an extremely high level of versatility thanks to the possibility of switching from a CR configuration to a CCK configuration with the same system. This allows the surgeon to choose the best configuration in the field without the need
for additional instruments.
Dr. Franz:
The instruments are actually very user-friendly, not only for the surgeon, but also for the OR nurses and the entire OR team. They are easy to maintain, easy to clean and easy to use. The number of instruments required is low and they are versatile.
Prof. Matziolis:
Instruments have a significant impact on surgical satisfaction. At the end of the day, clinical outcome and implant survival depend leastwise on the positioning as well as on the design of the implant. The LSK instruments are very well designed and allow for easy and efficient handling during surgery. The instruments are designed to be comfortable and functional.
Is there any part of the instruments that you particularly like?
Prof. Matziolis:
One instrument that I particularly like is the distal femoral cut guide, which can be adjusted to the exact degree. This allows for proper adjustment in extra-articular deformities or special cases. It also allows precise control of the distal femoral resection, which is not offered by all instruments on the market. Another instrument I appreciate is the tibial resection control instrument. It allows parallax-free axis control by guiding the rod to the ankle. These instruments allow precise control of the resections, which I strive to achieve with near-navigational precision.
What are the advantages of the LinkSymphoKnee being available with PorEx surface modification?
Dr. Franz:
PorEx contributes to a comprehensive system, as there are always patients who have a metal intolerance. By including this option, there’s no need to switch to a new system.
Prof. Matziolis:
Although only a small percentage of our patients report an allergy, we take it seriously and use coated implants when necessary. LSK is very advantageous in this regard because I don’t have to change my surgical technique or instruments. I can just use a different coated implant without having to go through an additional learning curve.
Dr. Calafiore:
It is great that the LINIK PorEx version is available for all configurations, which gives the surgeon more security in case of problems or uncertain history, and thanks to this possibility, our clinic will be able to treat different pathologies with a single prosthetic system.

LinkSymphoKnee CCK version with LINK PorEx* (available for each configuration).
* LINK PorEx:TiNbN=Titanium-Niobium-Nitride;
surface modification (gold color)
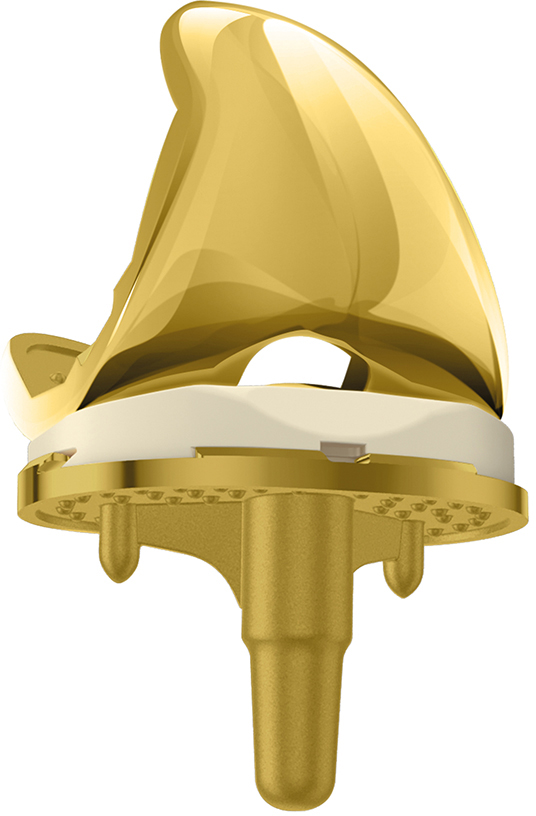
The LinkSymphoKnee is available in 14 femoral and 10 tibial sizes. All configurations are approved for 2-up, 2-down size compatibility. E-DUR (highly cross-linked PE with antioxidant vitamin E) is available for the articular surfaces and the patella. The picture shows the CR version with LINK PorEx* surface modification.
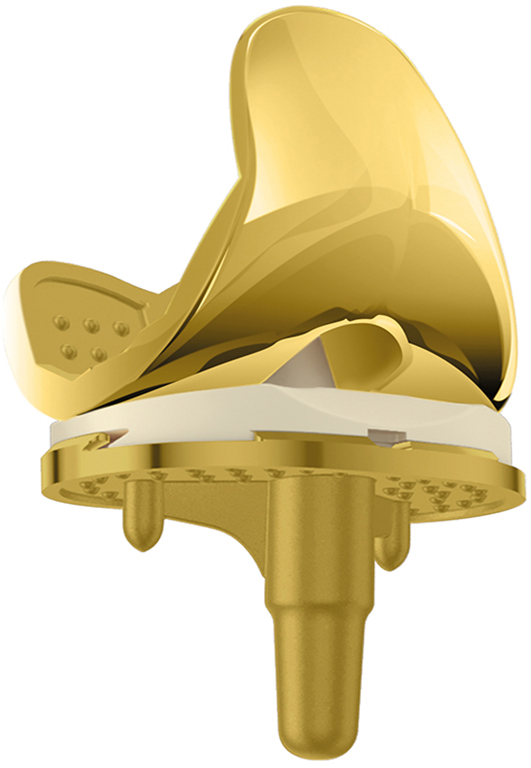
The LinkSymphoKnee is a complete system for primary and revision solutions. The picture shows the PS version with LINK PorEx* (available for each configuration).

The articulating surface of the LinkSymphoKnee All-Poly is identical to the PS insert.
How was the transition from your previous system to the LinkSymphoKnee?
Dr. Calafiore:
The LSK instrumentation is clear and simple, and the technology is complete and intuitive, so the learning curve is faster than with other systems used in the past. These features also allow healthcare professionals to perform procedures in the operating room to support the surgeon with greater safety and agility. In my personal experience, I had immediate confidence in the system and the instruments, which led to great postoperative satisfaction.
Prof. Matziolis:
Our clinic has maintained the extension-gap-first surgical philosophy. However, the LSK instruments are designed to accommodate many other surgical philosophies. Although there was a learning curve, the transition was relatively smooth because we were already using the SPAR-K instrumens with the GEMINI SL Total Knee Replacement from LINK. The instruments are designed to be user-friendly, so it was easy to get started with the new system.
Dr. Franz:
The learning curve was manageable because I was heavily involved in the instrumentation design. We were able to carefully consider and discuss each step and explain exactly why and where certain features should or should not be used. In our hospital, we implemented the LSK system on January 1, 2022, and the team was trained on the new system within a few days. It has proven to be easy to understand and learn, even for novice or less experienced surgeons.
How well do the LINK Endo-Model and the LinkSymphoKnee work together?
Prof. Matziolis:
With the CC system, we need to implant fewer Endo-Models. I am gaining initial experience with the CCK version of the LSK, which is relatively new to the market. The advantage is that it uses the same instruments and allows specific instrumentation for intramedullar gui-dance when using uncemented stems. If you are using cemented stems, you can also use the primary instruments to place the CC. I think in the future we will do some of the implantations that we used to do with the Endo-Model Rotating Hinge Knee with the CCK because the instrumentation is very simple. In addition, the patella tracking may be better with the CCK than with the Rotating Hinge Knee because it limits the rotation between the femur and and tibia by the CC conformity, which allows the patella to glide better. However, we need to study and confirm this further. The Endo-Model remains indicated for cases with complete collateral ligament loss. The CCK is appropriate for patients with preserved but insufficient medial ligament.
Dr. Calafiore:
The Endo-Model system integrates perfectly with the resections of the first implant, thanks to its unique radius of curvature and the 3 mm metal thickness of the condylar surface. The main indication that leads me to choose this system is in cases of significant instability of the joint, i.e. when there is a loss of a collateral ligament, an instability of the medial capsule, or when we cannot manage a space in flexion versus a space in extension.
Dr. Franz:
The CCK system is an important intermediate step between the CR system and the LINK Endo-Model. For severe deformities that cannot be treated with a CCK, you would start with the EndoModel first. There are gradations from the CR to the CCK and finally to the Endo-Model. For severe deformities, I would go immediately with the Endo-Model. Whenever the flexion-
extension gap cannot be balanced, a change to the Endo-Model is necessary. With the LSK system, LINK is offering a CCK component for the first time. In the past, we had limited options and had to rely on other systems. With the introduction of the LSK system, we now have access to a wider range of options, which may result in fewer fully constrained knees being required.
Have you had a case where the LSK system solved a specific problem that might not have been easily solved with other systems?
Prof. Matziolis:
I can’t give you a specific case, but the LSK has advantages, especially with the PS-Plus inlay, which allows for easy semi-constrain without additional stem lengthening. If we feel that something is too loose, we can simply insert a PS-Plus inlay to resolve the situation quickly and elegantly. This is something we use regularly and has contributed to the popularity of the implant.
Dr. Franz:
A major advantage of the LSK system is that I can use the PS-Plus system during surgery for minor instabilities, such as varus or valgus, without having to work on the overall construct or require stem fixation. This provides greater flexibility and allows for better customization to the individual needs of the patient. A case where the LSK system provided a great intraoperative advantage was when I identified a major medial cruciate ligament injury during a standard primary knee surgery, which immediately led me to opt for a CCK component. The addition of just one tray to the ones already in the field allowed me to complete the surgery without any problems or waste any time that would have caused possible infections.
Dr. Calafiore:
In recent months, I have seen significant medial collateral ligament damage in primary knee reconstructions, requiring the use of a more limited CCK prosthesis. The presence of the LSK complex system was fundamental, because with some additional tools already available, I was able to complete the operation without hesitation, without wasting time that could have caused possible infections, always keeping the patient’s health in mind.
Does the LSK system speed up the patient’s recovery?
Dr. Franz:
A patient who was previously operated on with another system had persistent discomfort and limited range of motion. By switching to the LSK system, we were able to optimize the patellofemoral kinematics and improve flexion function. After surgery and appropriate rehabilitation, the patient quickly noticed a significant improvement in flexion and a significant reduction in pain. This allowed him to recover faster and return to normal activity sooner than expected.
Does the LSK affect your workflow?
Dr. Calafiore:
In this first year of continuous use of the LSK system, I have had excellent experiences, due to the rapid recovery of the patient in the postoperative phase, especially in the case of direct loading: the patient feels secure without any sensation of instability of the joint. All this is possible thanks to an important study on the femoral trochlea, from which a design of the femoral component was derived that allows excellent flexion just a few days after surgery. The possibility of having the LSK instrument set within the hospital structure, which allows almost all configurations, optimizes and facilitates the processes of request and delivery to suppliers, saving work and time for the professionals in charge of carrying out this work.
How would you summarize your first postoperative results with the LSK system?
Dr. Franz:
The results were comparable or better than with other systems. In particular, the flexion function has proven to be very good due to the improved design. Both users and patients have given very positive feedback. In our clinic we have used more than 300 LSK implants so far.
Prof. Matziolis:
Our initial clinical experience with LSK has been very good throughout. Patients are able to bend well very early on, but we have not yet done a comparative study.
Dr. Calafiore:
The postoperative results have been excellent, with patients able to bear full weight shortly after surgery – even the same day. There have been no postoperative problems, which indicates a smooth and efficient recovery process. Most importantly, I have not seen any complications associated with the use of the implant over the medium to long term. This demonstrates the safety and effectiveness of the implant in facilitating a quick return to normal activity.
How did you find working with the international surgeons in the development group?
Dr. Franz:
Very stimulating, because we had very different approaches and were able to integrate them into the system. The LSK system is not a purely German system, but an international prosthesis system. Especially the topic of CCK was historically more relevant in America than the Endo-Model was in Germany or Central Europe. By working together, we were able to combine different aspects and experiences. We benefited from each other and were able to develop an innovative and versatile system that offers many advantages for both surgeons and patients.

Prof. Dr. med. Georg Matziolis
is Medical Director at the Waldkliniken Eisenberg, Chief Physician at the Clinic for Orthopedics and Trauma Surgery, and Professor of Orthopedics at the University Hospital Jena, Eisenberg Campus, Germany. Prof. Matziolis is a member of the international LinkSymphoKnee development group.

Dr. Giuseppe Calafiore, MD
is a Consultant Surgeon, Knee and Hip Replacement at the Clinica Città di Parma and the Parma Clinic Humanitas Rozzano in Milan, Italy. Dr. Calafiore is a member of the international LinkSymphoKnee development group.

Dr. Alois Franz
is Medical Director of the Hospital of Orthopedic Surgery and Sportmedicine at the St Marienkrankenhaus Siegen, Germany, a certified Maximum Care Center for Arthroplasty. Dr. Franz is a member of the international LinkSymphoKnee development group.

More information about LinkSymphoKnee System can be found via the QR code shown or via linksymphoknee.com