Revision of a rotationally unstable tibial component with individual TrabecuLink tibial hybrid cone in an epi-metaphyseal defect
Case Report: directLINK 1/2020
After the primary implantation of a knee joint prosthesis in 2003, an inlay change in 2004 and a revision of the knee prosthesis in 2011, due to implant loosening, to a LINK Endo-Model rotational knee prosthesis with tibial LinkSpacer, the patient presented in 2017 due to persistent discomfort. The X-ray examination revealed a renewed loosening of the tibial, while the diagnostic arthrocentesis revealed nothing abnormal. Since the primary care clinic refused another revision due to the complexity of the procedure, the patient was referred to the Orthopedic Clinic of the Hanover Medical School in the DIAKOVERE Annastift.
While X-ray diagnostics showed tibial implant loosening and a patella baja, the femoral part of the prosthesis was firmly anchored radiologically and scintigraphically; a knee arthrocentesis again showed no microbial evidence. Clinically, a non-irritant healed scar without any sign of infection was found with a pronounced intraarticular effusion, which was seen in an X-ray image with predominantly dorsal synovial thickening. The extension/flexion was 0–5–95°.
Because the quality of life of the patient, who was 180cm tall and 96kg in weight, was severely impaired, and because of the loosening of the implant, a revision was indicated. The firmly anchored femoral part of the implant was to be retained and the rotationally unstable tibial component changed.
Massive uncovered epiphyseal defect makes the use of a standard implant unrealistic.
The strategy for the revision was to create a rotationally stable metadiaphyseal anchorage for the prosthesis with reconstruction of the epiphysis. However, due to the massive uncovered epiphyseal defect, this could not be achieved with the standard implant. CustomLINK therefore fabricated a custzomized press-fit tibia hybrid cone that could be anchored in the metaphysis largely without cement, and into which the prosthesis stem was cemented. Due to the patella baja, and in order to reduce the patella impingement, the joint line was shifted tibially by 5mm to caudal.
Tibia hybrid cone with »barrier« to seal off the cement.
The tibial hybrid cone, which is partly cementless with the TrabecuLink structure in the bone and partly smooth on the outside in the area of the missing cortex of the tibial head, has an internal »barrier«, like the standard cones to seal off the cement with which the prosthesis stem was cemented. A channel in the smooth cone area allows an optional cerclage for additional stabilization. The caudal cutout on the cone allows the stem to be passed through.
The preoperative planning was implemented intraoperatively without any restrictions. The good primary stability of the tibial hybrid cone made it possible to dispense with an additional extension of the prosthesis socket.
No postoperative complications; very good pain reduction.
Initially there were no postoperative complications. The patient was mobilized early and achieved a flexion of 90° after only a few days. The postoperative X-ray findings were normal. A hematoma infection after three weeks with the detection of Staphylococcus aureus led to dry and irritation-free wound conditions after a single wound revision with inlay change and antibiotics. Afterwards, a complication-free progress without indication of infection persistence was observed.
The patient currently describes a very good pain reduction compared to the preoperative situation without the use of analgesics.
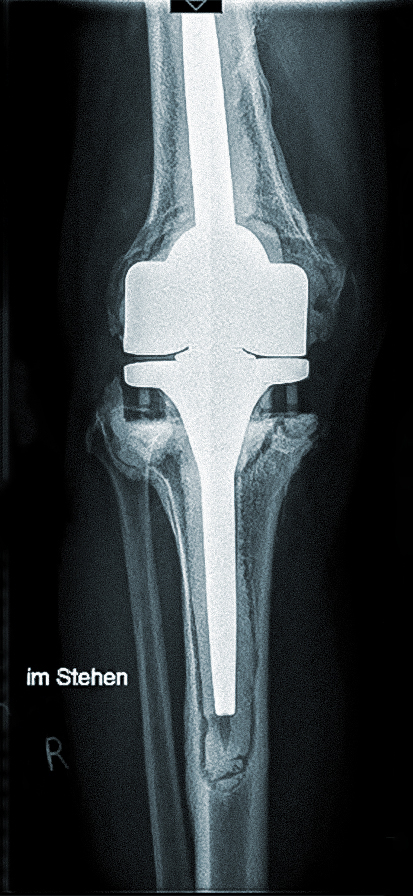
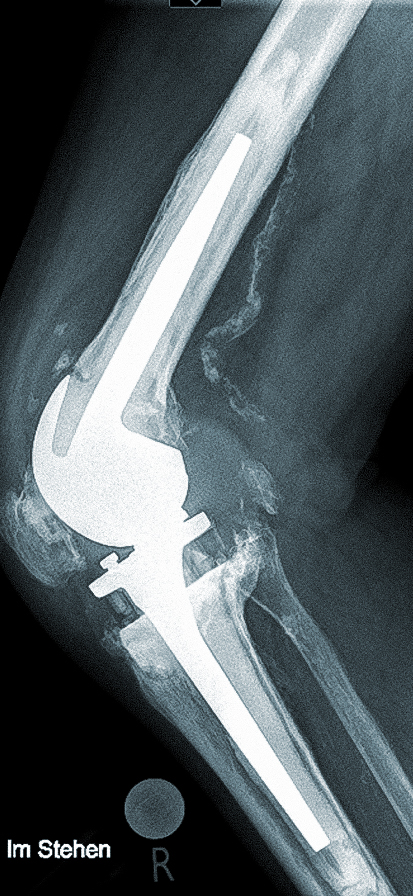
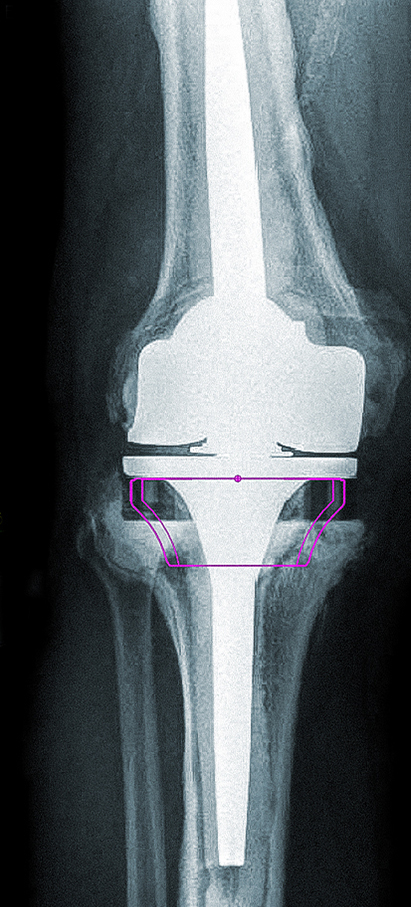
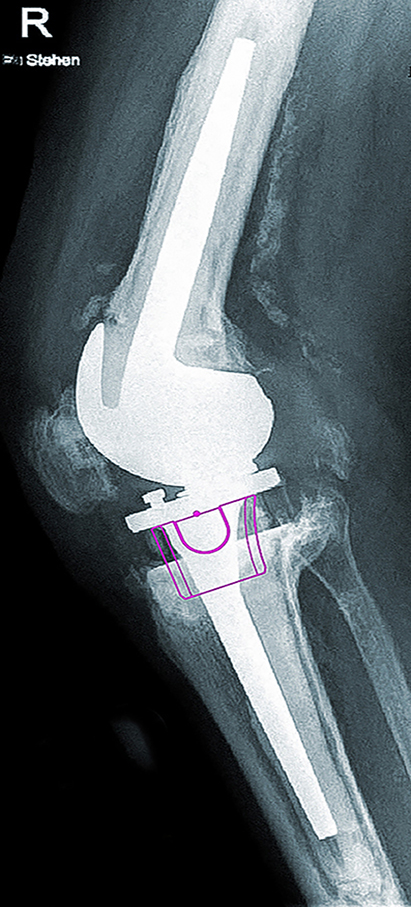
Preoperative X-rays show a revision knee prosthesis with a correct fit and clear signs of loosening in the tibia and the retropatellar replacement (1, 2); planning approach with a standard tibial cone, which proved to be too small in the largest available version (3, 4).




CT-based planning from tibial cone of customLINK with TrabecuLink surface (blue zones) for cementless anchorage (1); tibial cone from customLINK with TrabecuLink coating (2), rear, lateral and front view; customized shape-matching additive printed compressor (3, 4).
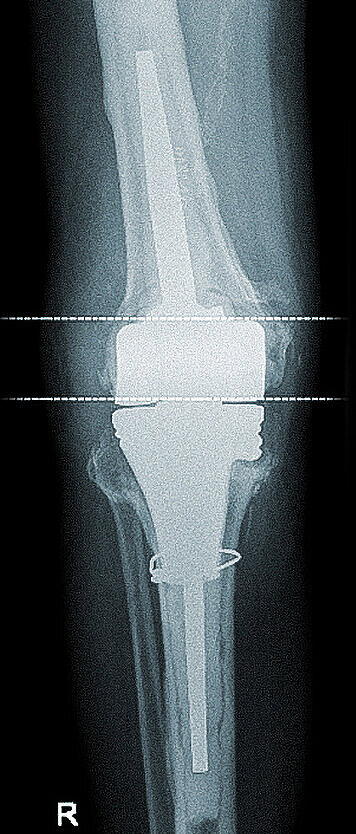

X-rays AP and lateral six weeks postoperatively: correct position of the revision prosthesis with physiological patella articulation; good press-fit of the metaphyseal tibial component; prophylactically applied securing cerclage (1, 2).
Contact: PD Dr. Tilman Calliess